
Introduction
Neurological disorders: here’s a number that should stop you—one in eight people on this planet is living with a neurological disorder right now. That’s over a billion human beings dealing with something going wrong in their brain, spinal cord, or nerve pathways, often every single day. Seizures. Tremors. Pain that doesn’t quit. Memory slipping. Balance failing.
And a huge portion of them aren’t getting enough relief from standard medications. Not because they haven’t tried — they have. It’s just that the brain is extraordinarily complicated, and most drugs are blunt tools applied to very precise problems.
That’s the context behind why medical cannabis has become one of the most actively researched areas in neurology. Not as a cure. Not as magic. But as a family of compounds—cannabinoids—that interact with a receptor system woven throughout the very tissue that neurological diseases damage.
We see this play out in clinic every week. Someone with MS still dealing with brutal spasticity despite multiple medications. A patient with Parkinson’s who can’t sleep through the night. A parent asking whether CBD is safe for treatment-resistant epilepsy. This guide gives clear, research-grounded answers to those questions.
So What Exactly Is a Neurological Disorder?
Short version: it’s any condition where the nervous system stops working the way it should. That includes your brain, your spinal cord, and all those nerves threading out to your fingertips and toes.
Longer version: neurological disorders are diseases caused by structural damage, electrical misfiring, biochemical imbalances, immune attacks, or genetic errors in neural tissue. They’re different from purely psychological conditions in one important way—with a neurological disorder, there’s something measurably wrong with the tissue, the signaling, or the chemistry. That measurability matters for diagnosis and treatment.
You’ll see these conditions called lots of things depending on who’s writing: brain disorders, nervous system diseases, neurologic conditions, CNS disorders, neurodegenerative diseases (when the damage is progressive). The terminology shifts, but the core idea doesn’t. Something is interfering with how nerve cells talk to each other, grow, or stay alive.
The Eight Main Categories
| Category | Description | Examples |
|---|---|---|
| 🧠 Neurodegenerative | Neurons progressively die over time. These conditions worsen and are not currently reversible. | Alzheimer’s, Parkinson’s, ALS, Huntington’s |
| ⚡ Seizure Disorders | Caused by abnormal electrical activity in the brain, leading to seizures. | Epilepsy, Dravet syndrome, Lennox-Gastaut |
| 🛡️ Autoimmune / Inflammatory | The immune system mistakenly attacks the nervous system. | Multiple sclerosis, Guillain-Barré |
| 🧬 Genetic / Rare | Linked to gene mutations, often rare but lifelong conditions. | Rett syndrome, Tourette disorder, Friedreich’s ataxia |
| 🤕 Traumatic | Physical injury damages the brain or spinal cord, disrupting function. | Traumatic brain injury (TBI), spinal cord injury |
| 👶 Pediatric / Developmental | Appear early in life and affect brain development and function. | Cerebral palsy, ADHD, autism-related neurological conditions |
| 🩺 Functional (FND) | Real neurological symptoms without visible structural damage; affects brain network function. | Tremors, paralysis, non-epileptic seizures |
| 😴 Sleep-Neurological | Disorders linked to neurological control of sleep cycles and behavior. | Narcolepsy, REM behavior disorder, restless legs syndrome |
One thing worth saying plainly: the line between neurology and psychiatry is blurrier than medical textbooks suggest. Patients ask us, “Is OCD a neurological disorder?” Is bipolar disorder neurological? Is fibromyalgia? All three show measurable brain circuit differences on imaging. All three sit at the intersection of what we call “neuro” and what we call “psych.” That overlap matters because it shapes which treatments get offered and which ones get ignored.
Which Neurological Disorders Are Most Common in America?
The 2024 JAMA Neurology analysis of the US nervous system burden gave us the clearest picture we’ve had. Here’s what it showed, in plain numbers:
Then there are the rare neurological disorders in adults—conditions like ALS (roughly 30,000 Americans at any moment), stiff-person syndrome, and neuromyelitis optica. Numerically small. Individually catastrophic. And precisely the group where conventional medicine has the least to offer, which is why alternative and adjunct therapies matter so much to these patients.
Symptoms That Should Send You Straight to a Doctor
The tricky thing about neurological symptoms is how varied they are. A seizure is unmistakable. But the early signs of MS? They might look like “just being tired” for months. That delay in recognition is part of why neurological diagnoses often take years to arrive.
“What neurological disorders cause balance problems” is one of the highest-searched neurological queries in the US, and it’s a fair one. Balance failure is often the first visible sign of something wrong. The culprits include:
- Multiple sclerosis—demyelination disrupts the motor coordination pathways running through the spinal cord and cerebellum
- Neurological walking disorders from cerebellar damage or peripheral neuropathy—the gait becomes unsteady, wide-based, or shuffling
- Parkinson’s disease—postural instability is a core feature, not just tremors
- Toe walking as a neurological disorder — often a sign of spastic cerebral palsy or sensory processing abnormalities in children
- Central vertigo—when true vertigo comes from the brainstem or cerebellum rather than the inner ear, it’s neurological and warrants urgent imaging

Nine Warning Signs That Demand Prompt Evaluation
- A sudden, severe headache you’ve never felt before—neurologists call it a “thunderclap headache,” and it’s an emergency until proven otherwise
- New confusion, memory gaps, or personality shifts appearing over days or weeks
- One-sided weakness or numbness — the classic stroke presentation
- Vision changes: double vision, sudden loss in one eye, visual field cuts
- Difficulty swallowing (dysphagia as a neurological disorder signal) or sudden speech changes
- Unexplained seizures or episodes of uncontrolled movement
- Progressive tremor, rigidity, or slowness of movement
- Significant sleep disruption—neurological sleep disorders, including REM behavior disorder, where patients physically act out dreams, are often early markers of Parkinson’s
- Balance or coordination failing without obvious cause
Neurological Disorders in Children: Different Disease, Different Stakes
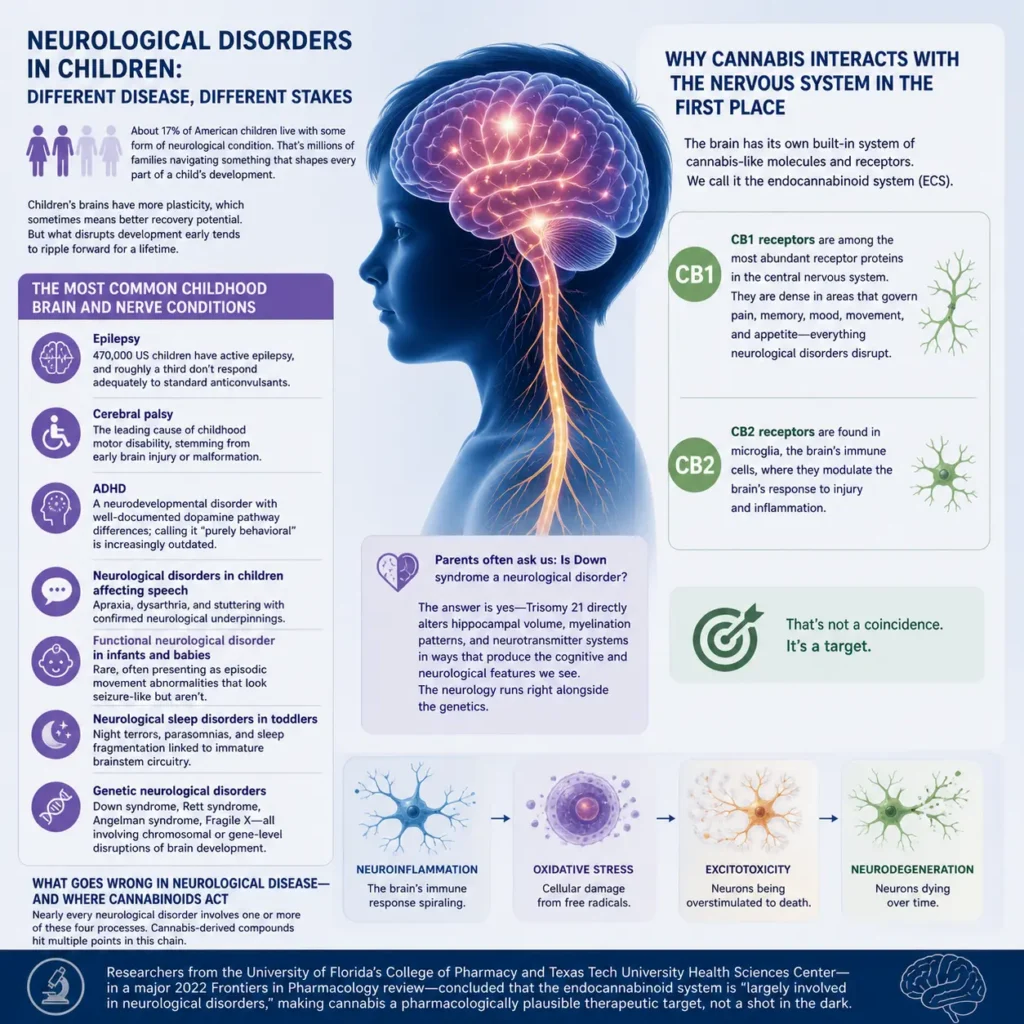
About 17% of American children live with some form of neurological condition. That’s not a rounding error — that’s millions of families navigating something that shapes every part of a child’s development.
Pediatric neurological disorders differ from adult-onset conditions in important ways. Children’s brains have greater plasticity, which sometimes means better potential for recovery. But it also means that what disrupts development early tends to ripple forward for a lifetime.
The Most Common Childhood Brain and Nerve Conditions
- Epilepsy—470,000 US children have active epilepsy, and roughly a third don’t respond adequately to standard anticonvulsants
- Cerebral palsy — the leading cause of childhood motor disability, stemming from early brain injury or malformation
- ADHD — a neurodevelopmental disorder with well-documented dopamine pathway differences; calling it “purely behavioral” is increasingly outdated
- Neurological disorders in children affecting speech — apraxia, dysarthria, and stuttering with confirmed neurological underpinnings
- Functional neurological disorder in infants and babies — rare, often presenting as episodic movement abnormalities that look seizure-like but aren’t
- Neurological sleep disorders in toddlers — night terrors, parasomnias, and sleep fragmentation linked to immature brainstem circuitry
- Genetic neurological disorders—Down syndrome, Rett syndrome, Angelman syndrome, Fragile X—all involving chromosomal or gene-level disruptions of brain development
Parents often ask us: Is Down syndrome a neurological disorder? The answer is yes — Trisomy 21 directly alters hippocampal volume, myelination patterns, and neurotransmitter systems in ways that produce the cognitive and neurological features we see. The neurology runs right alongside the genetics.
Why Cannabis Interacts With the Nervous System in the First Place
This is the piece most people haven’t heard explained properly. Cannabis works on the nervous system not because it’s an external drug forcing its way in — but because the brain has its own built-in system of cannabis-like molecules and receptors. We call it the endocannabinoid system (ECS).
The ECS has two main receptor types. CB1 receptors are among the most abundant receptor proteins in the entire central nervous system. They sit densely in regions that govern pain perception, memory, mood, movement, and appetite, which is basically a list of everything neurological disorders disrupt. CB2 receptors were originally thought to live only in immune tissue. We now know they’re also present in microglia, the brain’s own immune cells—and that they modulate the brain’s response to injury and inflammation.
That’s not a coincidence. It’s a target.
What Goes Wrong in Neurological Disease — And Where Cannabinoids Act
Nearly every neurological disorder involves one or more of these four processes: neuroinflammation (the brain’s immune response spiraling), oxidative stress (cellular damage from free radicals), excitotoxicity (neurons being overstimulated to death), and neurodegeneration (neurons dying over time). Cannabis-derived compounds hit multiple points in this chain.
This is why researchers from the University of Florida’s College of Pharmacy and Texas Tech University Health Sciences Center — in a major 2022 Frontiers in Pharmacology review — concluded that the endocannabinoid system is “largely involved in neurological disorders,” making cannabis a pharmacologically plausible therapeutic target, not a shot in the dark.
What the Research Actually Shows — Condition by Condition
Let’s be honest about the state of the evidence. It’s uneven. Some conditions have strong, regulatory-level clinical trial data. Others have promising early signals. And some have very little. Here’s where things actually stand as of 2026:
Epilepsy: This Is Where the Evidence Is Clearest
Epidiolex — a pharmaceutical-grade purified CBD — earned FDA approval in 2018 for Dravet syndrome and Lennox-Gastaut syndrome. These aren’t obscure conditions with soft endpoints. These are devastating childhood epilepsies where kids can have dozens of seizures a day and parents live in permanent terror.
In Phase III trials, Epidiolex cut monthly seizure frequency by roughly 39% to 54% versus placebo. About half of patients hit the clinical benchmark of a 50% or greater reduction. For a condition where nothing else was working, that’s not a minor result.
A 2026 review from the University of Beira Interior confirmed CBD’s benefits extend to other refractory pediatric epilepsies and autism-associated seizures. The evidence base keeps growing.
Multiple Sclerosis: Conclusive for Spasticity
MS is the most searched neurological condition in the US by a wide margin — 301,000 searches a month. And it’s where cannabis medicine has its second-strongest evidence base.
Nabiximols (Sativex® — a 1:1 THC:CBD oromucosal spray) has regulatory approval in over 30 countries specifically for MS-related spasticity, backed by Phase III RCTs. The peer-reviewed classification? “Conclusive.” That’s the highest evidence tier. Not “promising.” Not “emerging.” Conclusive.
Beyond spasticity, MS patients consistently report using medical cannabis for neuropathic pain, bladder dysfunction, sleep problems, and mood. Each of those symptoms has a neurological mechanism — and MS’s core pathology (immune attack on the myelin sheath) aligns with CBD’s known anti-inflammatory effects through CB2 receptor modulation.
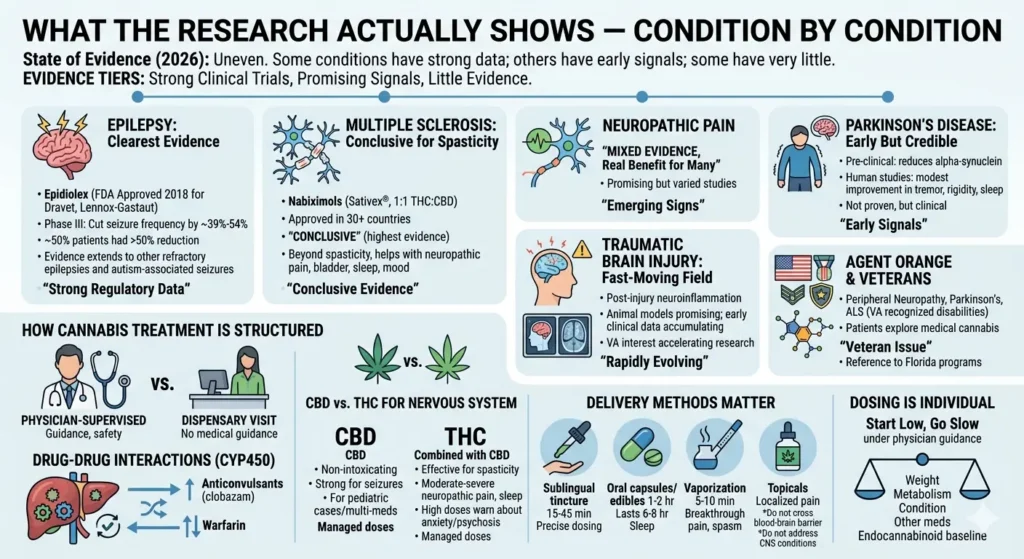
Neuropathic Pain: Mixed Evidence, Real Benefit for Many
Parkinson’s Disease: Early But Credible
Pre-clinical studies suggest cannabinoids may reduce the accumulation of alpha-synuclein — the protein that forms toxic Lewy bodies. There are also early human studies on tremor, rigidity, and Parkinson’s-related sleep disorders that show modest improvement with cannabis. It’s not a proven treatment for Parkinson’s. But for patients already dealing with limited options and significant non-motor symptoms, cannabis is increasingly part of the clinical conversation.
Traumatic Brain Injury: A Fast-Moving Field
TBI gets 5,400 searches a month — and for good reason. Post-injury neuroinflammation is a primary driver of secondary brain damage in the weeks after a head injury. CBD’s anti-inflammatory profile has shown promise in animal models, and early clinical case data is accumulating. The VA’s growing interest in cannabis for combat-related TBI has accelerated human research considerably.
Agent Orange and Neurological Disorders: A Veteran Issue
Veterans exposed to Agent Orange carry elevated rates of peripheral neuropathy, Parkinson’s disease, and ALS — all VA-recognized service-connected disabilities. Many of these patients are now exploring medical cannabis as an adjunct to conventional care. Florida’s medical cannabis program covers chronic pain, PTSD, ALS, and Parkinson’s, which makes Venice Care Clinic a natural fit for veterans in Southwest Florida.
How Cannabis Treatment Is Actually Structured for Patients with Neurological Disorders
Here’s where we need to be direct with you. There’s a big difference between what you’d get at a physician-supervised medical cannabis clinic and what you’d get from a dispensary visit without any medical guidance.
Neurological patients — almost by definition — are on other medications. Anticonvulsants. Immunosuppressants. Blood thinners. Antidepressants. CBD is metabolized through the liver’s CYP450 system, the same pathway that handles many of those drugs. Without physician oversight, you can inadvertently raise the blood levels of anticonvulsants like clobazam to dangerous concentrations. You can interact with warfarin. These aren’t theoretical concerns — they’re documented drug-drug interactions.
CBD vs. THC — Which One for Nervous System Disorders?
CBD (cannabidiol) is non-intoxicating, has the strongest evidence for seizure disorders, and is where most physicians start for neurological patients — particularly those on other medications and particularly in pediatric cases.
THC, in carefully managed low doses combined with CBD, is more effective for spasticity (as in MS) and moderate-to-severe neuropathic pain. It also helps with sleep, which matters enormously for patients with neurological sleep disorders. The key word is managed. High-THC products can worsen anxiety and trigger psychotic episodes in people predisposed to those reactions.
Delivery Method Matters More Than People Realize in Neurological Disorders
- Sublingual tinctures — onset in 15–45 minutes. Most precise dosing control. Good daily foundation.
- Oral capsules and edibles — 1–2 hours to kick in, but effects last 6–8 hours. Best for neurological sleep disorders where overnight coverage is the goal.
- Vaporization — 5–10 minute onset. Useful for breakthrough pain or acute spasm. Not ideal for anyone with respiratory compromise.
- Topicals — helpful for localized peripheral nerve pain. Don’t cross the blood-brain barrier, so they don’t address CNS-level neurological conditions directly.
And dosing? It’s individual. Body weight, liver metabolism, severity of condition, concurrent medications, and individual endocannabinoid baseline all affect response. This is why the standard approach is “start low, go slow” — under physician guidance, not from a YouTube recommendation.
What Qualifies in Florida? Neurological Conditions Under the Medical Cannabis Program
Florida’s medical marijuana law covers a broader range of conditions than many patients realize. Neurological disorders are at the heart of the qualifying list:
- Epilepsy and seizure disorders
- Multiple sclerosis
- Parkinson’s disease
- ALS (amyotrophic lateral sclerosis)
- Chronic neuropathic pain
- PTSD (with its documented neurobiological basis)
- Glaucoma (via optic nerve involvement)
- Terminal conditions including brain tumors
- Crohn’s disease (neurological gut-brain axis connection)
- “Other debilitating conditions” — determined by physician evaluation
That last category — other debilitating conditions — is significant. Functional neurological disorder, rare neurological disorders in adults, neurological sleep disorders, and genetic neurological disorders may all qualify when a licensed physician documents meaningful functional impairment. It’s not a blanket exemption—it requires a proper clinical evaluation. That’s exactly what we do.
| 🧠 Condition | 📌 Qualifies in Florida | 🔍 Clinical Notes |
|---|---|---|
| Epilepsy & Seizure Disorders | ✅ Yes | Strongest evidence base; CBD commonly used |
| Multiple Sclerosis (MS) | ✅ Yes | Approved for spasticity; helps pain, sleep, bladder issues |
| Parkinson’s Disease | ✅ Yes | Early evidence; used for tremor, rigidity, sleep |
| ALS (Amyotrophic Lateral Sclerosis) | ✅ Yes | Recognized debilitating neurological condition |
| Chronic Neuropathic Pain | ✅ Yes | Mixed evidence; widely used clinically |
| PTSD | ✅ Yes | Neurological basis; affects brain function and stress response |
| Glaucoma | ✅ Yes | Optic nerve involvement; pressure-related nerve damage |
| Terminal Conditions (e.g. Brain Tumors) | ✅ Yes | Includes severe neurological decline |
| Crohn’s Disease | ✅ Yes | Gut-brain axis involvement; neurological component |
| Other Debilitating Conditions | ⚠️ Case-by-case | Requires physician evaluation and documented impairment |
Is Medical Cannabis Safe for Neurological Patients? The Honest Answer
Yes, with appropriate caveats. Cannabis isn’t the same risk profile as opioids. There’s no lethal dose. But it’s also not harmless, particularly in neurological contexts.
The Real Risks Worth Knowing
- Drug interactions are the most pressing concern for neurological patients, specifically. CBD raises blood levels of some anticonvulsants. If you’re on clobazam, valproate, or warfarin, you need physician monitoring—not guesswork.
- High-THC products and psychiatric side effects — THC can worsen anxiety and, in predisposed individuals, trigger psychotic episodes. For patients where OCD or bipolar disorder overlaps with neurological symptoms, this needs careful assessment.
- Cognitive effects with heavy THC use — regular high-dose THC is associated with short-term memory effects. For patients with dementia or significant cognitive vulnerability, THC doses should be very conservative.
- Respiratory risk from smoking — medical use should avoid combustion. Vaporization and non-inhalation routes are clinically preferred.
Conclusion
Neurological disorders are hard. Fundamentally, stubbornly hard. The brain is the most complicated organ in the known universe, and when things go wrong inside it — whether it’s Alzheimer’s quietly stripping memory, MS attacking the myelin sheath, or epilepsy sending electrical storms through a child’s developing brain — medicine still has enormous blind spots.
Medical cannabis isn’t filling all those blind spots. But it’s filling something. FDA-approved CBD for childhood epilepsy isn’t a fringe claim — it’s regulatory science. Phase III trial data for MS spasticity isn’t anecdotal—it’s clinical evidence. The endocannabinoid system threading through neural tissue isn’t a coincidence — it’s a biological target that researchers are actively and productively exploring.
What we ask patients at our clinic is simple: are you getting enough relief from what you’re currently doing? If the answer is no — and for a lot of neurological patients, it honestly is — then a proper evaluation of whether medical cannabis could help is worth having. Not from a dispensary clerk. From a physician who understands both the evidence and your specific situation.
That’s what we do at Venice Care Clinic. If you’re in Florida and living with a neurological condition, we’re here.
Frequently Asked Questions
What neurological disorders cause balance problems?
Multiple sclerosis, Parkinson’s disease, cerebellar ataxia, vestibular neuritis, and peripheral neuropathy are the most common culprits. Neurological walking disorders — gait imbalance caused by nerve or brain damage — affect hundreds of thousands of Americans. Balance problems are often the earliest visible sign of something more serious. If your balance has shifted without obvious explanation, a neurology evaluation shouldn’t wait.
Can medical cannabis actually help with neurological disorders?
For specific conditions, the evidence is solid. Epidiolex (FDA-approved CBD) reduces seizures in Dravet syndrome by roughly 50% in clinical trials. Nabiximols (THC+CBD) has Phase III data for MS spasticity. A 2025 review of 22 RCTs found consistent positive results for neuropathic pain. Beyond those, there’s credible early evidence for Parkinson’s, TBI, and several rare conditions. The strength varies by diagnosis — which is why individualized evaluation matters.
What counts as a rare neurological disorder?
Conditions affecting fewer than 200,000 Americans. ALS, Huntington’s disease, Creutzfeldt-Jakob disease, neuromyelitis optica, stiff-person syndrome, and progressive supranuclear palsy are among the most recognized. These patients often carry the highest individual burden—the conditions are severe, and conventional options are thin. A 2026 review found meaningful early cannabinoid evidence in several rare conditions, including Tourette disorder and certain refractory epilepsies.
Is OCD a neurological disorder?
It’s at the neurological-psychiatric intersection. Brain imaging consistently shows abnormalities in the cortico-striato-thalamo-cortical circuit in people with OCD. Many neurologists now treat it as a brain network disorder rather than a purely behavioral one. Similarly, bipolar disorder and fibromyalgia both show measurable brain-level differences that blur the neurology/psychiatry line. Cannabis research for OCD specifically is limited and complicated by THC’s anxiety-altering properties.
What is a functional neurological disorder (FND)—and is it real?
Very real. FND causes genuine tremors, paralysis, speech problems, and non-epileptic seizures in patients who have no structural brain lesion on imaging. It’s not malingering or “in the head.” Current research shows FND involves abnormal connectivity between brain networks responsible for voluntary movement and attention. It’s present in up to 30% of neurology outpatient caseloads—making it one of the most common yet under-discussed neurological conditions in the US.
Can neurological disorders qualify you for medical cannabis treatment in Florida?
Yes. Many neurological conditions may qualify under Florida’s medical marijuana program, including epilepsy, Parkinson’s disease, multiple sclerosis, neuropathy, chronic migraines, and other conditions causing persistent neurological symptoms. A licensed medical cannabis doctor evaluates your symptoms, medical history, and treatment needs to determine eligibility.
How can a cannabis clinic help with neurological disorders?
A cannabis clinic helps patients manage symptoms linked to neurological disorders such as chronic pain, muscle stiffness, tremors, sleep problems, seizures, anxiety, and nerve discomfort. Medical cannabis doctors create personalized treatment plans based on your condition, symptom severity, and response to previous therapies.
Where can I find a medical cannabis doctor near Venice, Florida?
Patients searching for a cannabis clinic or medical cannabis doctors near Venice, FL can schedule an evaluation at Venice Care. The clinic provides medical cannabis evaluations for qualifying neurological conditions and guidance on Florida medical marijuana card eligibility.