
Introduction
Crohn’s disease is a chronic inflammatory bowel condition affecting an estimated 3.1 million adults in the United States (CDC, 2025). If you live in Venice, Sarasota County, or anywhere in Florida and are searching for evidence-based answers — from infusion therapy to diet changes to medical cannabis — this guide covers everything you need to know.
What Is Crohn’s Disease?
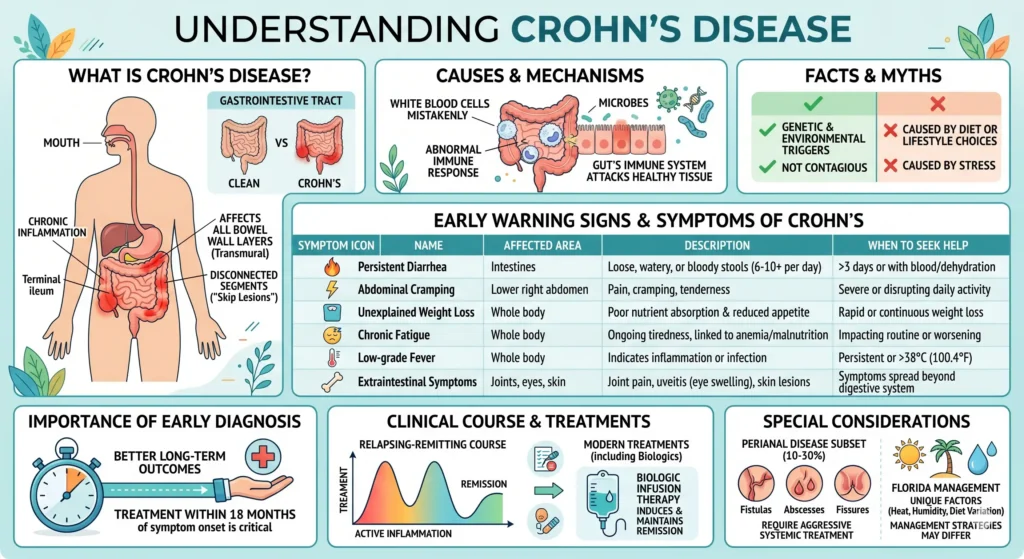
Crohn’s disease is a chronic, relapsing inflammatory bowel disease (IBD) that causes inflammation anywhere along the entire gastrointestinal (GI) tract—from the mouth to the anus. Unlike ulcerative colitis, which is limited to the colon’s inner lining, Crohn’s disease can affect all layers of the bowel wall and may involve multiple disconnected segments (“skip lesions”).
The condition is believed to result from an abnormal immune response in genetically predisposed individuals, triggered by environmental and microbial factors. The gut’s immune system attacks healthy intestinal tissue, producing chronic inflammation, ulceration, and structural damage over time.
Crohn’s disease is not caused by diet, stress, or poor lifestyle choices—though these factors can influence flare-up frequency. It is also not contagious. In Florida, where heat, humidity, and diet variation are unique factors, disease management strategies may differ slightly from national guidelines.
Clinical definition
Crohn’s disease is a chronic transmural inflammatory disease of the GI tract, most commonly affecting the terminal ileum and colon. It is characterized by a relapsing–remitting course, with periods of active inflammation alternating with remission. No definitive cure currently exists, but modern treatments — including biologics delivered via infusion — can induce and maintain long-term remission in many patients.
Early Warning Signs and Symptoms of Crohn’s Disease
Symptoms vary significantly by the location of inflammation in the GI tract. The most common form—ileocolonic Crohn’s—primarily affects the end of the small intestine (terminal ileum) and the beginning of the large intestine. Early diagnosis is critical: patients who receive treatment within 18 months of symptom onset have significantly better long-term outcomes than those diagnosed later.
| Symptom | Severity Level | Frequency | Affected Area | Description | When to Seek Help |
|---|---|---|---|---|---|
| 🔥 Persistent diarrhea | Moderate to Severe | Daily during flare | Intestines | Loose, watery, or bloody stools, often 6–10+ times per day. | If lasting >3 days or with blood/dehydration. |
| ⚡ Abdominal cramping | Mild to Severe | Frequent | Lower right abdomen (ileum) | Pain, cramping, or tenderness due to intestinal inflammation. | If severe or disrupting daily activity |
| ⚖️ Unexplained weight loss | Moderate | Gradual | Whole body | Caused by poor nutrient absorption and reduced appetite. | If rapid or continuous weight loss |
| 😴 Chronic fatigue | Moderate to Severe | Persistent | Whole body | Ongoing tiredness linked to anemia, inflammation, and malnutrition. | If impacting routine or worsening |
| 🌡️ Low-grade fever | Mild to Moderate | Occasional | Whole body | Indicates active inflammation or possible infection. | If persistent or above 38°C |
| 🦴 Extraintestinal symptoms | Varies | Intermittent | Joints, eyes, skin | Includes joint pain, uveitis, skin lesions, and inflammation outside the gut. | If symptoms spread beyond digestive system |
Approximately 10–30% of Crohn’s patients develop perianal disease, which includes fistulas, abscesses, and fissures around the anus. This subset of patients typically requires more aggressive systemic treatment, often including biologic infusion therapy.
How Is Crohn’s Disease Diagnosed?
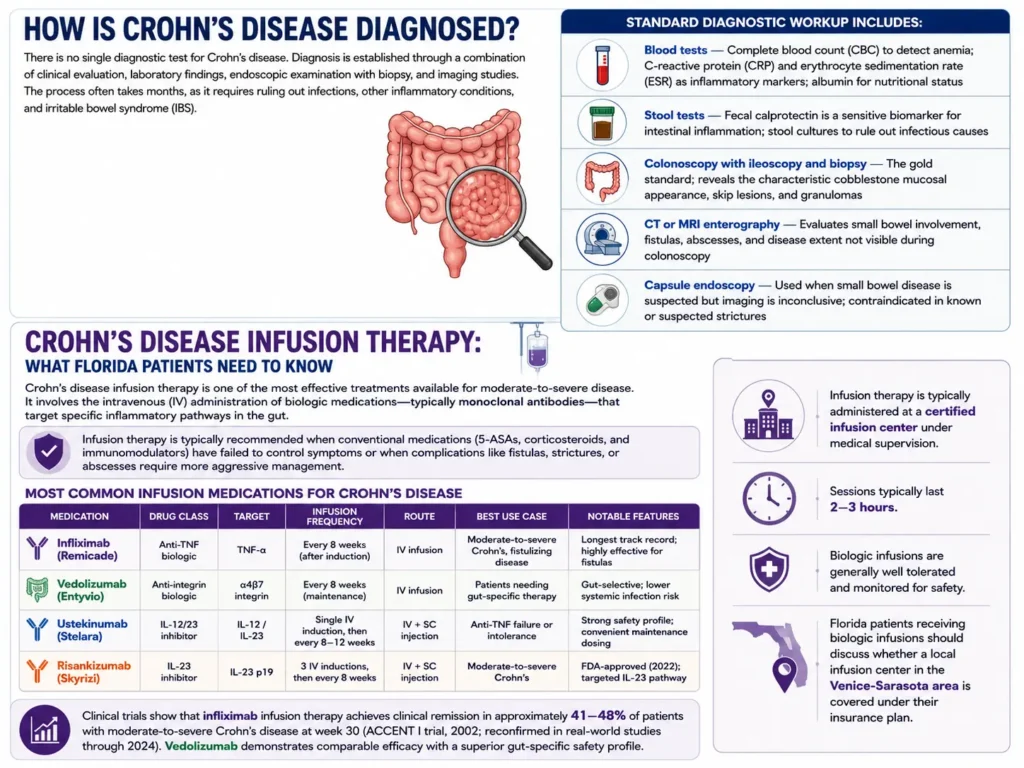
There is no single diagnostic test for Crohn’s disease. Diagnosis is established through a combination of clinical evaluation, laboratory findings, endoscopic examination with biopsy, and imaging studies. The process often takes months, as it requires ruling out infections, other inflammatory conditions, and irritable bowel syndrome (IBS).
Standard diagnostic workup includes:
- Blood tests — Complete blood count (CBC) to detect anemia; C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) as inflammatory markers; albumin for nutritional status
- Stool tests — Fecal calprotectin is a sensitive biomarker for intestinal inflammation; stool cultures to rule out infectious causes
- Colonoscopy with ileoscopy and biopsy — The gold standard; reveals the characteristic cobblestone mucosal appearance, skip lesions, and granulomas
- CT or MRI enterography—Evaluates small bowel involvement, fistulas, abscesses, and disease extent not visible during colonoscopy
- Capsule endoscopy — Used when small bowel disease is suspected but imaging is inconclusive; contraindicated in known or suspected strictures
Crohn’s Disease Infusion Therapy: What Florida Patients Need to Know
Crohn’s disease infusion therapy is one of the most effective treatments available for moderate-to-severe disease. It involves the intravenous (IV) administration of biologic medications—typically monoclonal antibodies—that target specific inflammatory pathways in the gut.
Infusion therapy is typically recommended when conventional medications (5-ASAs, corticosteroids, and immunomodulators) have failed to control symptoms or when complications like fistulas, strictures, or abscesses require more aggressive management.
Most Common Infusion Medications for Crohn’s Disease
| Medication | Drug Class | Target | Infusion Frequency | Route | Best Use Case | Notable Features |
|---|---|---|---|---|---|---|
| Infliximab (Remicade) | Anti-TNF biologic | TNF-α | Every 8 weeks (after induction) | IV infusion | Moderate-to-severe Crohn’s, fistulizing disease | Longest track record; highly effective for fistulas |
| Vedolizumab (Entyvio) | Anti-integrin biologic | α4β7 integrin | Every 8 weeks (maintenance) | IV infusion | Patients needing gut-specific therapy | Gut-selective; lower systemic infection risk |
| Ustekinumab (Stelara) | IL-12/23 inhibitor | IL-12 / IL-23 | Single IV induction, then every 8–12 weeks | IV + SC injection | Anti-TNF failure or intolerance | Strong safety profile; convenient maintenance dosing |
| Risankizumab (Skyrizi) | IL-23 inhibitor | IL-23 p19 | 3 IV inductions, then every 8 weeks | IV + SC injection | Moderate-to-severe Crohn’s | FDA-approved (2022); targeted IL-23 pathway |
Clinical trials show that infliximab infusion therapy achieves clinical remission in approximately 41–48% of patients with moderate-to-severe Crohn’s disease at week 30 (ACCENT I trial, 2002; reconfirmed in real-world studies through 2024). Vedolizumab demonstrates comparable efficacy with a superior gut-specific safety profile.
Infusion therapy is typically administered at a certified infusion center under medical supervision. Sessions typically last 2–3 hours. Florida patients receiving biologic infusions should discuss whether a local infusion center in the Venice-Sarasota area is covered under their insurance plan.
Full Treatment Options for this Disease
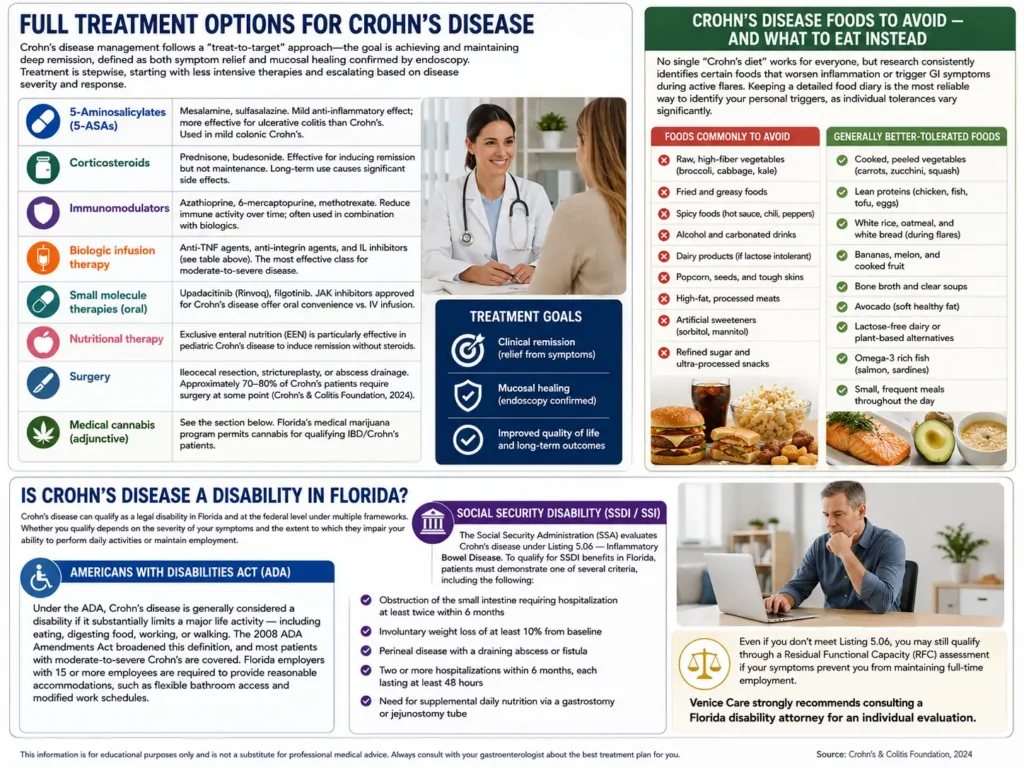
Crohn’s disease management follows a “treat-to-target” approach—the goal is achieving and maintaining deep remission, defined as both symptom relief and mucosal healing confirmed by endoscopy. Treatment is stepwise, starting with less intensive therapies and escalating based on disease severity and response.
- 5-Aminosalicylates (5-ASAs) — Mesalamine, sulfasalazine. Mild anti-inflammatory effect; more effective for ulcerative colitis than Crohn’s. Used in mild colonic Crohn’s.
- Corticosteroids — Prednisone, budesonide. Effective for inducing remission but not maintenance. Long-term use causes significant side effects.
- Immunomodulators — Azathioprine, 6-mercaptopurine, methotrexate. Reduce immune activity over time; often used in combination with biologics.
- Biologic infusion therapy—Anti-TNF agents, anti-integrin agents, and IL inhibitors (see table above). The most effective class for moderate-to-severe disease.
- Small molecule therapies (oral) — Upadacitinib (Rinvoq), filgotinib b. JAK inhibitors approved for Crohn’s disease offer oral convenience vs. IV infusion.
- Nutritional therapy — Exclusive enteral nutrition (EEN) is particularly effective in pediatric Crohn’s disease to induce remission without steroids.
- Surgery — Ileocecal resection, strictureplasty, or abscess drainage. Approximately 70–80% of Crohn’s patients require surgery at some point (Crohn’s & Colitis Foundation, 2024).
- Medical cannabis (adjunctive)—See the section below. Florida’s medical marijuana program permits cannabis for qualifying IBD/Crohn’s patients.
Crohn’s Disease Foods to Avoid — and What to Eat Instead
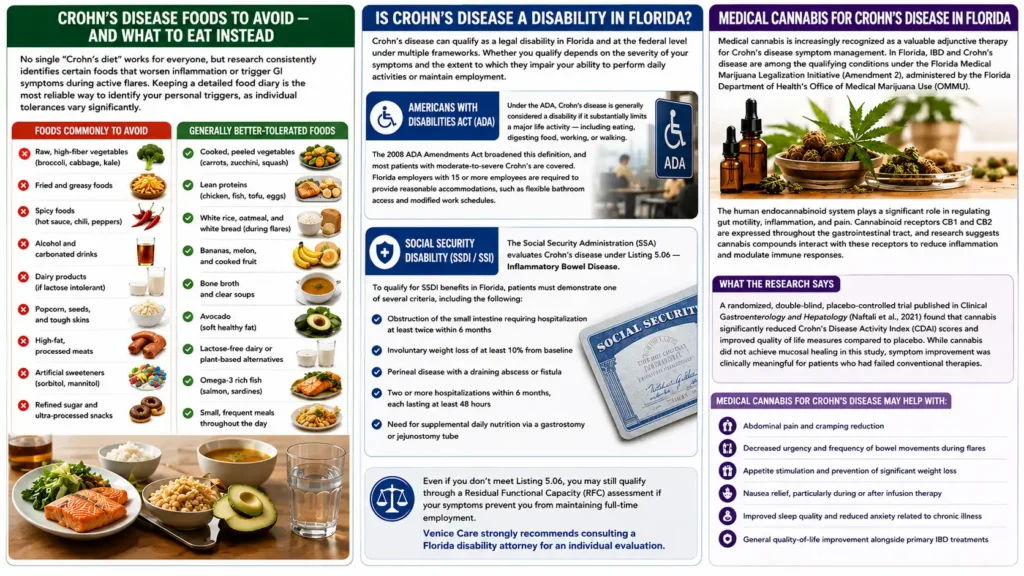
No single “Crohn’s diet” works for everyone, but research consistently identifies certain foods that worsen inflammation or trigger GI symptoms during active flares. Keeping a detailed food diary is the most reliable way to identify your personal triggers, as individual tolerances vary significantly.
- Raw, high-fiber vegetables (broccoli, cabbage, kale)
- Fried and greasy foods
- Spicy foods (hot sauce, chili, peppers)
- Alcohol and carbonated drinks
- Dairy products (if lactose intolerant)
- Popcorn, seeds, and tough skins
- High-fat, processed meats
- Artificial sweeteners (sorbitol, mannitol)
- Refined sugar and ultra-processed snacks
- Cooked, peeled vegetables (carrots, zucchini, squash)
- Lean proteins (chicken, fish, tofu, eggs)
- White rice, oatmeal, and white bread (during flares)
- Bananas, melon, and cooked fruit
- Bone broth and clear soups
- Avocado (soft healthy fat)
- Lactose-free dairy or plant-based alternatives
- Omega-3 rich fish (salmon, sardines)
- Small, frequent meals throughout the day
Is Crohn’s Disease a Disability in Florida?
Crohn’s disease can qualify as a legal disability in Florida and at the federal level under multiple frameworks. Whether you qualify depends on the severity of your symptoms and the extent to which they impair your ability to perform daily activities or maintain employment.
Americans with Disabilities Act (ADA)
Under the ADA, Crohn’s disease is generally considered a disability if it substantially limits a major life activity — including eating, digesting food, working, or walking. The 2008 ADA Amendments Act broadened this definition, and most patients with moderate-to-severe Crohn’s are covered. Florida employers with 15 or more employees are required to provide reasonable accommodations, such as flexible bathroom access and modified work schedules.
Social Security Disability (SSDI / SSI)
The Social Security Administration (SSA) evaluates Crohn’s disease under Listing 5.06 — Inflammatory Bowel Disease. To qualify for SSDI benefits in Florida, patients must demonstrate one of several criteria, including the following:
- Obstruction of the small intestine requiring hospitalization at least twice within 6 months
- Involuntary weight loss of at least 10% from baseline
- Perineal disease with a draining abscess or fistula
- Two or more hospitalizations within 6 months, each lasting at least 48 hours
- Need for supplemental daily nutrition via a gastrostomy or jejunostomy tube
Even if you don’t meet Listing 5.06, you may still qualify through a Residual Functional Capacity (RFC) assessment if your symptoms prevent you from maintaining full-time employment. Venice Care strongly recommends consulting a Florida disability attorney for an individual evaluation.
Medical Cannabis for Crohn’s Disease in Florida
Medical cannabis is increasingly recognized as a valuable adjunctive therapy for Crohn’s disease symptom management. In Florida, IBD and Crohn’s disease are among the qualifying conditions under the Florida Medical Marijuana Legalization Initiative (Amendment 2), administered by the Florida Department of Health’s Office of Medical Marijuana Use (OMMU).
The human endocannabinoid system plays a significant role in regulating gut motility, inflammation, and pain. Cannabinoid receptors CB1 and CB2 are expressed throughout the gastrointestinal tract, and research suggests cannabis compounds interact with these receptors to reduce inflammation and modulate immune responses.
What the Research Says
A randomized, double-blind, placebo-controlled trial published in Clinical Gastroenterology and Hepatology (Naftali et al., 2021) found that cannabis significantly reduced Crohn’s Disease Activity Index (CDAI) scores and improved quality of life measures compared to placebo. While cannabis did not achieve mucosal healing in this study, symptom improvement was clinically meaningful for patients who had failed conventional therapies.
Medical cannabis for Crohn’s disease may help with:
- Abdominal pain and cramping reduction
- Decreased urgency and frequency of bowel movements during flares
- Appetite stimulation and prevention of significant weight loss
- Nausea relief, particularly during or after infusion therapy
- Improved sleep quality and reduced anxiety related to chronic illness
- General quality-of-life improvement alongside primary IBD treatments
Crohn’s Disease Care in Venice, Florida — How Venice Care Can Help
Venice Care, led by Dr. Barry Gordon, MD, is a compassionate healthcare practice located in Venice, Florida, serving patients across Sarasota County and the greater Venice area. While our primary specialty is medical cannabis evaluation and certification for qualifying conditions, we work closely with gastroenterologists and IBD specialists throughout Sarasota and Charlotte counties to provide coordinated Crohn’s disease care.
At Venice Care, we help Crohn’s patients in two key ways:
- Medical marijuana certification—We evaluate whether Crohn’s disease or IBD qualifies you for Florida’s Medical Marijuana program, provide the required physician certification, and support your application with the OMMU.
- Compassionate, integrative care — We help patients understand all their symptom management options, including the role of cannabis alongside conventional therapies like infusion treatment, dietary management, and stress reduction.
Frequently Asked Questions About Crohn’s Disease
What is Crohn’s disease infusion therapy?
Crohn’s disease infusion therapy delivers biologic medications directly into the bloodstream through an intravenous (IV) line. Common options include infliximab (Remicade) and vedolizumab (Entyvio).
Infusions are typically given every 4–8 weeks at a certified infusion center and are used for moderate-to-severe Crohn’s disease that hasn’t responded to oral treatments. Each session lasts about 2–3 hours and is performed under medical supervision.
What foods should you avoid with Crohn’s disease?
Common trigger foods include raw high-fiber vegetables, fried or greasy foods, spicy foods, alcohol, carbonated drinks, dairy (if lactose intolerant), and high-sugar processed snacks.
Triggers vary by individual. A 2–4 week food diary is the most reliable way to identify personal triggers. During flares, a low-residue diet helps reduce bowel frequency and abdominal cramping.
Is Crohn’s disease a disability in Florida?
Crohn’s disease can qualify as a disability under the Americans with Disabilities Act (ADA) if it significantly limits daily activities. It may also meet criteria for Social Security Disability Insurance (SSDI) under the SSA Digestive System Listing 5.06.
Florida residents may be eligible for workplace accommodations depending on symptom severity. Eligibility is determined case by case based on medical documentation and functional limitations.
Does medical cannabis help Crohn’s disease?
Medical cannabis may help manage symptoms such as abdominal pain, cramping, nausea, and appetite loss. Cannabinoids interact with CB1 and CB2 receptors in the gut, which influence inflammation and motility.
In Florida, Crohn’s disease and IBD can qualify patients for a medical marijuana card. Cannabis is typically used as supportive therapy—not a replacement for standard treatments.
What are the early warning signs of Crohn’s disease?
Early symptoms include persistent diarrhea (sometimes with blood or mucus); abdominal pain—often in the lower right abdomen; unexplained weight loss; fatigue; reduced appetite; and low-grade fever.
Some patients also develop mouth ulcers, skin issues, or joint pain before digestive symptoms appear. Early diagnosis improves long-term disease control and outcomes.
What is the difference between Crohn’s disease and ulcerative colitis?
Both are forms of inflammatory bowel disease (IBD), but they differ in scope:
- Crohn’s disease: Can affect any part of the GI tract; involves all layers of the bowel wall; often appears in patches (skip lesions)
- Ulcerative colitis: Limited to the colon and rectum; affects only the inner lining; continuous inflammation
These differences impact treatment approach and disease progression.
How do you get a medical marijuana card for Crohn’s disease in Florida?
To obtain a Florida medical marijuana card:
- Be a Florida resident with valid ID
- Receive a qualifying diagnosis from a licensed physician
- Get certified in the Florida OMMU registry
- Submit your application and $75 fee online
Once approved, you can purchase medical cannabis from licensed dispensaries in Florida.