
What Is Amyotrophic Lateral Sclerosis? A Plain-English Explanation
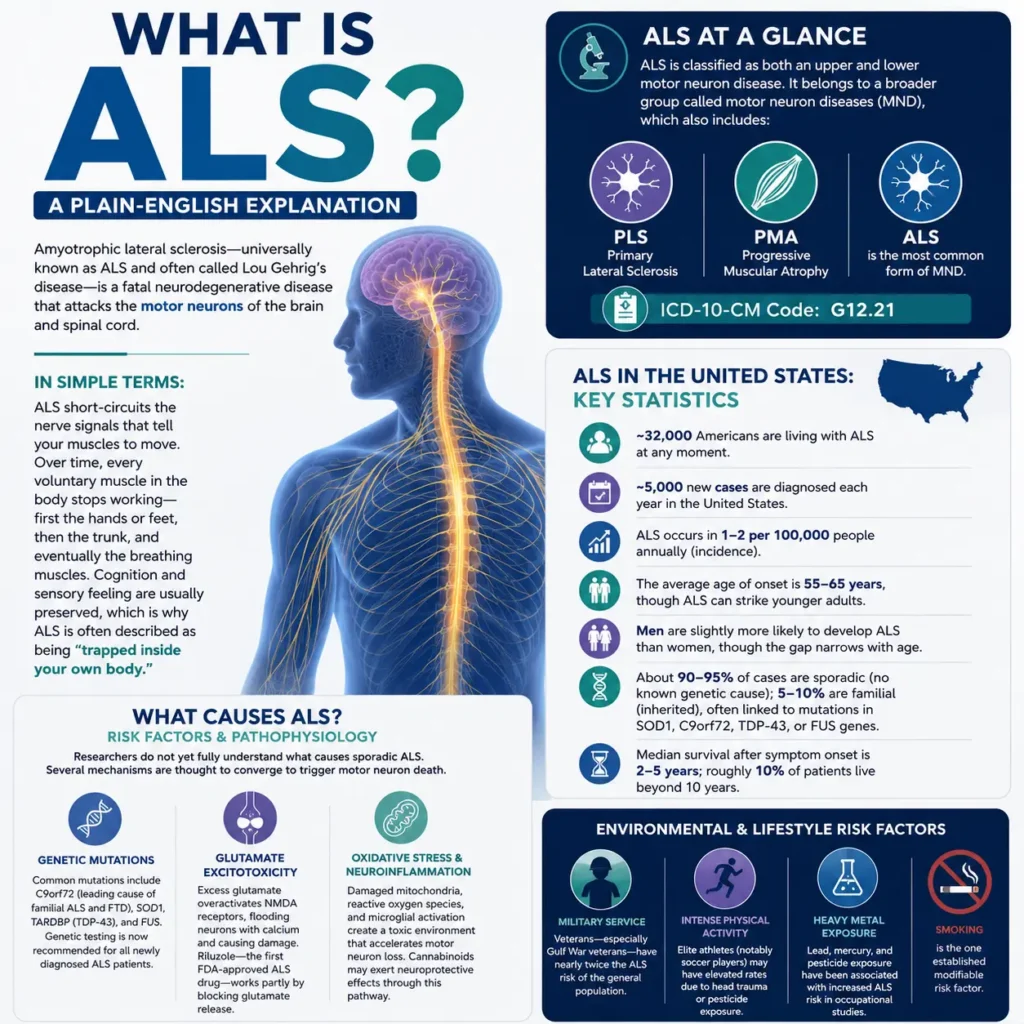
Amyotrophic lateral sclerosis—universally known as ALS and often called Lou Gehrig’s disease after the legendary Yankees first baseman who was diagnosed in 1939 — is a fatal neurodegenerative disease that attacks the motor neurons of the brain and spinal cord. The word itself breaks down like this: “a-myo-trophic” means “without muscle nourishment,” “lateral” refers to the spinal cord regions where motor neurons are located, and “sclerosis” means “hardening or scarring of tissue.”
Put simply: ALS short-circuits the nerve signals that tell your muscles to move. Over time, every voluntary muscle in the body stops working — first the hands or feet, then the trunk, and eventually the breathing muscles. Cognition and sensory feeling are usually preserved, which is why ALS is sometimes described as being “trapped inside your own body.”
🔬 ALS at a Glance
ALS is classified as both an upper and lower motor neuron disease. It belongs to a broader group called motor neuron diseases (MND), which also includes primary lateral sclerosis (PLS) and progressive muscular atrophy (PMA). ALS accounts for the majority of all MND diagnoses. The ICD-10-CM code for ALS is G12.21.
Amyotrophic Lateral Sclerosis in the United States: Key Statistics
ALS touches families in every state. According to the ALS Association and MDA, here is what the numbers look like across the USA:
- ~32,000 Americans are living with ALS at any moment.
- ~5,000 new cases are diagnosed each year in the United States.
- ALS occurs in 1–2 per 100,000 people annually (incidence).
- The average age of onset is 55–65 years, though ALS can strike younger adults.
- Men are slightly more likely to develop ALS than women, though the gap narrows with age.
- About 90–95% of cases are sporadic (no known genetic cause); 5–10% are familial (inherited), often linked to mutations in SOD1, C9orf72, TDP-43, or FUS genes.
- Median survival after symptom onset is 2–5 years; roughly 10% of patients live beyond 10 years.
What Causes Amyotrophic Lateral Sclerosis? Risk Factors & Pathophysiology
Researchers do not yet fully understand what causes sporadic ALS, which is why it remains one of neurology’s most urgent open questions. Several mechanisms are thought to converge to trigger motor neuron death.
Genetic Mutations
The most common genetic forms involve mutations in C9orf72 (the leading cause of familial ALS and frontotemporal dementia), SOD1, TARDBP (TDP-43), and FUS. Genetic testing is now recommended for all newly diagnosed ALS patients — especially because mutation-specific therapies like tofersen (for SOD1 mutations) are now FDA-approved.
Glutamate Excitotoxicity
Excess glutamate in the synapse is a key driver of motor neuron death in ALS. Glutamate overactivates NMDA receptors, flooding neurons with calcium and triggering cell damage. Riluzole — the first FDA-approved ALS drug — works partly by blocking glutamate release.
Oxidative Stress & Neuroinflammation
Damaged mitochondria, reactive oxygen species, and microglial activation create a toxic environment that accelerates motor neuron loss. This is also a pathway through which cannabinoids may exert neuroprotective effects (discussed later).
Environmental & Lifestyle Risk Factors
- Military service: Veterans — especially Gulf War veterans — have nearly twice the ALS risk of the general population.
- Intense physical activity: Some studies suggest elite athletes (notably soccer players) have elevated rates, possibly due to head trauma or pesticide exposure.
- Heavy metal exposure: Lead, mercury, and pesticide exposure have been associated with increased ALS risk in occupational studies.
- Smoking is the one established modifiable risk factor.
Early Signs & Symptoms of Amyotrophic Lateral Sclerosis (ALS)
Amyotrophic Lateral Sclerosis (ALS), also known as Lou Gehrig’s disease, is a progressive motor neuron disease (MND) that damages the nerve cells responsible for controlling voluntary muscles. Early symptoms of Amyotrophic Lateral Sclerosis vary depending on which motor neurons are affected first.
There are two primary forms of ALS onset:
- Limb-onset Amyotrophic Lateral Sclerosis — the most common type, beginning in the arms, hands, legs, or feet.
- Bulbar-onset ALS — starts in the muscles involved in speech and swallowing and affects approximately 25–30% of people diagnosed with Lou Gehrig’s disease.
Recognizing the early warning signs of ALS is important because symptoms of motor neuron disease often develop gradually and may initially appear mild.
✋ Muscle Weakness & Fasciculations
Progressive muscle weakness is one of the earliest and most common symptoms of Amyotrophic Lateral Sclerosis. Patients may notice weakness in one hand, arm, foot, or leg, difficulty gripping objects, frequent falls, or foot drop while walking. Muscle twitching, also called fasciculations, is another classic symptom of ALS and motor neuron degeneration.
🗣️ Slurred Speech (Dysarthria)
Speech changes are a major sign of bulbar-onset Amyotrophic Lateral Sclerosis. Speech may become slurred, slow, hoarse, or nasal-sounding as the muscles responsible for communication weaken.
🍽️ Swallowing Difficulty (Dysphagia)
Difficulty swallowing liquids or solid foods is common in progressive ALS. Many patients experience choking episodes, coughing during meals, prolonged eating times, and unexplained weight loss caused by dysphagia.
😤 Breathing Changes & Respiratory Symptoms
As Amyotrophic Lateral Sclerosis progresses, respiratory muscles may weaken, leading to shortness of breath, shallow breathing, and difficulty breathing while lying flat. Morning headaches and daytime fatigue can result from carbon dioxide retention during sleep.
😣 Muscle Cramps, Stiffness & Spasticity
Painful muscle cramps, stiffness, tight muscles, exaggerated reflexes, and spasticity are common neurological symptoms associated with upper motor neuron involvement in ALS.
😔 Fatigue, Anxiety & Emotional Changes
People living with Amyotrophic Lateral Sclerosis frequently experience persistent fatigue as muscle function declines. Emotional symptoms may include anxiety, depression, and pseudobulbar affect (PBA), which causes sudden uncontrollable laughing or crying.
⚠️ Delayed ALS Diagnosis
Diagnosing Amyotrophic Lateral Sclerosis can be challenging because early ALS symptoms often resemble other neurological disorders, including cervical myelopathy, multifocal motor neuropathy, multiple sclerosis (MS), and myasthenia gravis. For many patients, diagnosis may take 9–18 months or longer.
If you or a loved one develops progressive, painless muscle weakness, unexplained muscle twitching, speech problems, swallowing difficulty, or other symptoms of motor neuron disease, seek evaluation from a neurologist experienced in diagnosing Amyotrophic Lateral Sclerosis (ALS) as early as possible.
How Is Amyotrophic Lateral Sclerosis Diagnosed? Tests & Criteria
There is no single definitive test for ALS. Diagnosis is primarily clinical—meaning it is based on a neurologist’s assessment of signs and symptoms — but several investigations help confirm the picture and rule out other conditions.
El Escorial / Gold Coast Criteria (Amyotrophic Lateral Sclerosis)
The revised Gold Coast ALS diagnostic criteria (2020) require evidence of upper AND lower motor neuron signs in at least one body region, with progression over time, and no alternative diagnosis explaining the findings.
Key Diagnostic Tests
- Electromyography (EMG) & nerve conduction studies (NCS): The most important test — shows denervation in multiple body regions.
- MRI of the brain and spinal cord: Used to rule out structural causes; MRI findings in ALS (amyotrophic lateral sclerosis MRI) may show T2/FLAIR signal along the corticospinal tract.
- Blood and cerebrospinal fluid tests: To exclude mimicking conditions.
- Genetic testing: Increasingly standard; identifies actionable mutations (e.g., SOD1) that change treatment options.
- Pulmonary function tests: Vital for tracking respiratory decline and timing ventilatory support decisions.
- Neurofilament light chain (NfL) biomarker: An emerging blood/CSF biomarker showing promise for early diagnosis and tracking ALS progression.
The 7 Stages of ALS: Understanding Disease Progression
ALS is not a uniform disease — it progresses differently in every person. The most widely used staging framework describes 7 stages of ALS, from mildly symptomatic to complete loss of function. Understanding these stages helps patients and caregivers plan ahead and access the right support at the right time.
| Stage | Description | Key Features | Typical Care Needs |
|---|---|---|---|
| 1 | Diagnosis — Mild Symptoms | Weakness or fasciculations in one region; walking or fine motor changes | Neurologist; PT/OT assessment; genetic counseling |
| 2 | Moderate Weakness — One Region | Noticeable deficit in one area (e.g., foot drop or hand grip loss) | AFO braces, assistive devices; speech therapy if bulbar |
| 3 | Moderate Weakness — Two Regions | Spreading to a second body region; balance issues; fatigue | Wheelchair evaluation; nutritional support; respiratory monitoring |
| 4 | Severe Weakness — One Region | Complete loss of function in initial region; may still ambulate | Power wheelchair; AAC (augmentative communication) device |
| 5 | Severe Weakness — Two Regions | Dependent in most ADLs; significant bulbar or respiratory compromise | PEG feeding tube discussion; BiPAP/NIV; full-time caregiver |
| 6 | Loss of Speech or Swallowing | Non-oral feeding (PEG tube); AAC primary communication; possible tracheostomy | Palliative care integration; home ventilation; hospice planning |
| 7 | End-Stage ALS | Complete loss of voluntary movement; full ventilator dependency; locked-in state | Hospice; pain & symptom management; family support; VSED counseling |
The ALS progression timeline varies widely. Some patients move through all 7 stages in under two years; others plateau for extended periods. The bulbar-onset ALS stages often progress faster than limb-onset presentations. Tracking progression with the ALS Functional Rating Scale — Revised (ALSFRS-R) every 2–3 months gives patients and clinicians objective data for planning.
ALS Treatment Options in the USA: What’s Available in 2026
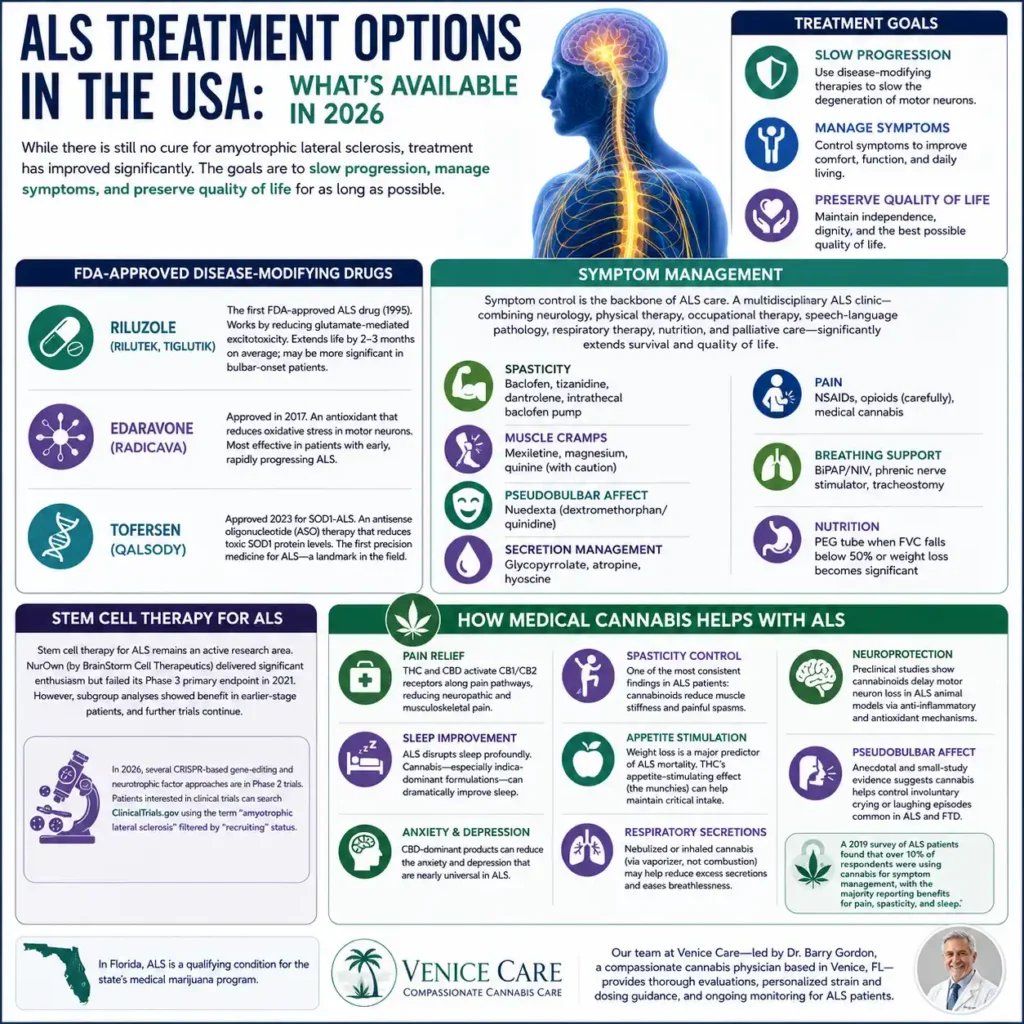
While there is still no cure for amyotrophic lateral sclerosis, treatment has improved significantly. The goals are to slow progression, manage symptoms, and preserve quality of life for as long as possible.
FDA-Approved Disease-Modifying Drugs
- Riluzole (Rilutek, Tiglutik): The first FDA-approved ALS drug (1995). Works by reducing glutamate-mediated excitotoxicity. Extends life by 2–3 months on average; may be more significant in bulbar-onset patients.
- Edaravone (Radicava): Approved in 2017. An antioxidant that reduces oxidative stress in motor neurons. Most effective in patients with early, rapidly progressing ALS.
- Tofersen (Qalsody): Approved 2023 for SOD1-ALS. An antisense oligonucleotide (ASO) therapy that reduces toxic SOD1 protein levels. The first precision medicine for ALS is a landmark in the field.
Symptom Management
Symptom control is the backbone of ALS care. A multidisciplinary ALS clinic—combining neurology, physical therapy, occupational therapy, speech-language pathology, respiratory therapy, nutrition, and palliative care—significantly extends survival and quality of life compared with standard neurology follow-up alone.
- Spasticity: Baclofen, tizanidine, dantrolene, intrathecal baclofen pump
- Muscle cramps: Mexiletine, magnesium, quinine (with caution)
- Pseudobulbar affect: Nuedexta (dextromethorphan/quinidine)
- Secretion management: Glycopyrrolate, atropine, hyoscine
- Pain: NSAIDs, opioids (carefully), medical cannabis (see below)
- Breathing support: BiPAP/NIV, phrenic nerve stimulator, tracheostomy
- Nutrition: PEG tube when FVC falls below 50% or weight loss becomes significant
Stem Cell Therapy for ALS
Stem cell therapy for ALS remains an active research area. NurOwn (by BrainStorm Cell Therapeutics) delivered significant enthusiasm but failed its Phase 3 primary endpoint in 2021. However, subgroup analyses showed benefit in earlier-stage patients, and further trials continue. In 2026, several CRISPR-based gene-editing and neurotrophic factor approaches are in Phase 2 trials. Patients interested in clinical trials can search ClinicalTrials.gov using the term “amyotrophic lateral sclerosis” filtered by “recruiting” status.
🌿 How Medical Cannabis Helps with Amyotrophic Lateral Sclerosis
At Venice Care, our compassionate cannabis clinic has served patients across Florida with personalized medical marijuana evaluations since our founding. For ALS patients, medical cannabis is one of the most promising complementary therapies available — and the science behind it is growing fast.
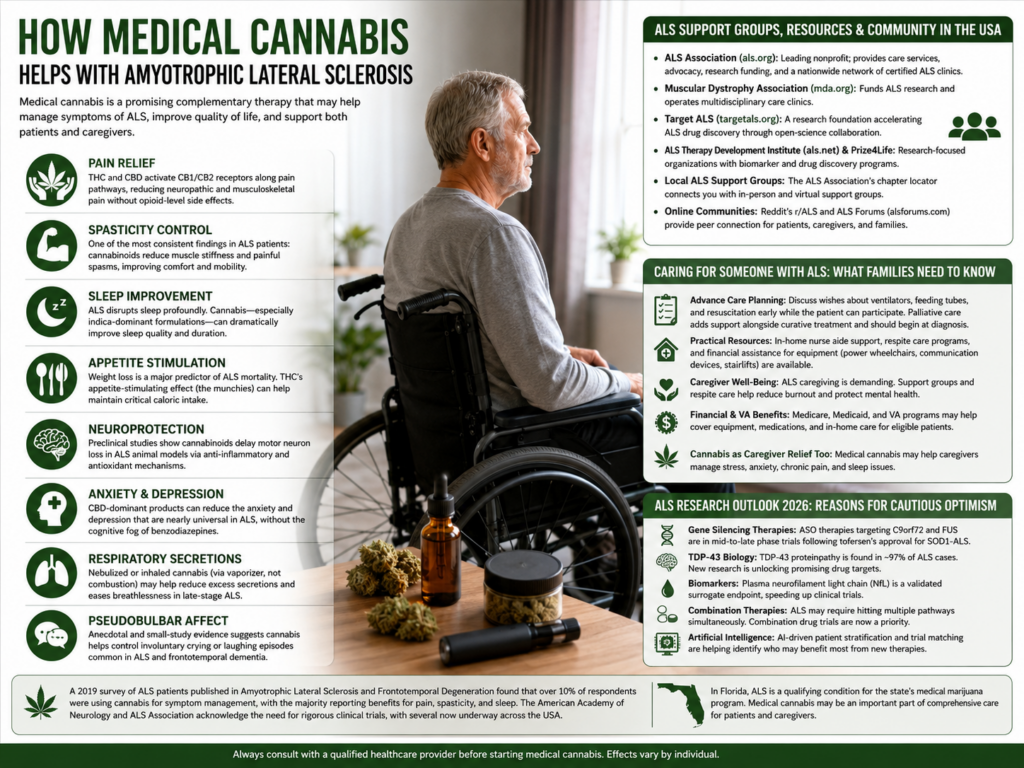
🩹 Pain Relief: THC and CBD activate CB1/CB2 receptors along pain pathways, reducing neuropathic and musculoskeletal pain without opioid-level side effects.
💪 Spasticity Control One of the most consistent findings in ALS patients: cannabinoids reduce muscle stiffness and painful spasms, improving comfort and mobility.
😴 Sleep Improvement ALS disrupts sleep profoundly. Cannabis — especially indica-dominant formulations — can dramatically improve sleep quality and duration.
🍽️ Appetite Stimulation Weight loss is a major predictor of ALS mortality. THC’s appetite-stimulating effect (the munchies) can help maintain critical caloric intake.
🧠 Neuroprotection: Preclinical studies show cannabinoids delay motor neuron loss in ALS animal models via anti-inflammatory and antioxidant mechanisms.
😰 Anxiety & Depression CBD-dominant products can reduce the anxiety and depression that are nearly universal in ALS, without the cognitive fog of benzodiazepines.
🫁 Respiratory Secretions Nebulized or inhaled cannabis (via vaporizer, not combustion) may help reduce excess secretions and eases breathlessness in late-stage ALS.
🗣️ Pseudobulbar Affect Anecdotal and small-study evidence suggests cannabis helps control involuntary crying or laughing episodes common in ALS and frontotemporal dementia.
What Current Research Says About Cannabis for ALS
A 2019 survey of ALS patients published in Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration found that over 10% of respondents were using cannabis for symptom management, with the majority reporting benefits for pain, spasticity, and sleep. The American Academy of Neurology and ALS Association both acknowledge the need for rigorous clinical trials, with several now underway across the USA.
In Florida, ALS is a qualifying condition for the state’s medical marijuana program. Our team at Venice Care — led by Dr. Barry Gordon, a compassionate cannabis physician based in Venice, FL — provides thorough evaluations, personalized strain and dosing guidance, and ongoing monitoring for ALS patients.
Amyotrophic Lateral Sclerosis Support Groups, Resources & Community in the USA
An ALS diagnosis changes everything — for the patient and for the whole family. The good news is that you are not alone. The United States has a rich ecosystem of ALS support groups, advocacy organizations, and multidisciplinary clinics.
- The ALS Association (als.org): The nation’s leading nonprofit; provides care services, walks, research funding, and a nationwide network of certified ALS clinics.
- Muscular Dystrophy Association (mda.org): Funds ALS research and runs multidisciplinary care clinics across the country.
- Target ALS (targetals.org): A research foundation accelerating ALS drug discovery through open-science collaboration.
- Prize4Life & ALS Therapy Development Institute (als.net): Research-focused organizations with biomarker and drug discovery programs.
- Local ALS support groups: The ALS Association’s chapter locator can connect you with in-person and virtual support groups. Florida has several active chapters.
- Online communities: Reddit’s r/ALS forum and the ALS Forums (alsforums.com) provide peer connections for patients, caregivers, and families.
Caring for Someone with ALS: What Families Need to Know
ALS caregiving is one of the most demanding roles in medicine. As the disease progresses through the 7 stages, care needs change rapidly—from simple assistance with activities of daily living in early stages to around-the-clock nursing in end-stage ALS.
Planning Ahead at Every Stage
Advance care planning — including documenting wishes about ventilator use, feeding tubes, and resuscitation — should begin early, while the patient can participate meaningfully. Palliative care is not the same as hospice; it is a layer of support that runs alongside curative-intent treatment and should begin at diagnosis.
Practical Caregiver Resources
- The ALS Association’s “Living With ALS” manual — a free, comprehensive caregiver guide
- In-home nurse aide support through Medicare/Medicaid and VA benefits for eligible veterans
- Respite care programs to give family caregivers regular breaks
- Financial assistance programs for ALS equipment (power wheelchairs, communication devices, stairlifts)
🌿 Cannabis as Caregiver Relief Too
Family caregivers of ALS patients experience extremely high rates of burnout, depression, and anxiety. Medical cannabis may offer supportive benefit for qualifying caregivers as well. Venice Care offers evaluations for a wide range of qualifying Florida conditions, including PTSD, chronic pain, and anxiety.
ALS Research Outlook 2026: Reasons for Cautious Optimism
The ALS research landscape in 2026 is more dynamic than at any point in the disease’s history. Several developments are generating real excitement:
- Gene silencing therapies: Following tofersen’s approval for SOD1-ALS, antisense oligonucleotide (ASO) therapies targeting C9orf72 and FUS are in mid-to-late Phase trials.
- TDP-43 biology: TDP-43 proteinopathy is found in ~97% of ALS cases. Understanding how TDP-43 misfolds and aggregates is unlocking new drug targets.
- Biomarkers: Plasma neurofilament light chain (NfL) is now validated as a surrogate endpoint in clinical trials, dramatically accelerating drug development timelines.
- Combination therapies: ALS, like cancer, may require hitting multiple pathways simultaneously. Trials testing drug combinations are now being prioritized.
- Artificial intelligence: AI-driven patient stratification and trial matching is helping identify which patients are most likely to benefit from which interventions—moving toward precision medicine for ALS.
How Venice Care Supports ALS Patients in Florida
Venice Care’s Amyotrophic Lateral Sclerosis department offers a compassionate, personalized approach to ALS support—with a particular focus on medical cannabis as a complementary therapy. We serve patients from across Florida, including Venice, Sarasota, North Port, Englewood, and surrounding areas.
Our founder, Dr. Barry Gordon, brings decades of clinical experience to patient-centered cannabis evaluations. We understand that every ALS patient’s journey is unique—which is why we take the time to understand your specific symptoms, stage of disease, current medications, and quality-of-life goals before making any recommendation.
Whether you are newly diagnosed and want to understand your options or you’re at a later stage and seeking better control of pain and spasticity, Venice Care is here for you. We also offer telehealth for patients who cannot travel.
Conclusion
Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, is a progressive motor neuron disease that affects muscle control, speech, swallowing, and breathing. While there is currently no cure for ALS, advances in neurological care, FDA-approved treatments, supportive therapies, and medical cannabis are helping improve symptom management and quality of life for many patients.
From early ALS symptoms like muscle weakness, fasciculations, dysphagia, and respiratory changes to advanced-stage care needs, early diagnosis and multidisciplinary treatment remain essential. At Venice Care, patients across Florida receive compassionate support, personalized medical marijuana evaluations, and guidance tailored to their unique ALS journey.
As research into amyotrophic lateral sclerosis, motor neuron disease, gene therapies, and neuroprotective treatments continues to evolve, there is growing hope for better outcomes and improved long-term care for people living with Lou Gehrig’s disease.
Frequently Asked Questions About Amyotrophic Lateral Sclerosis
What is the difference between ALS and multiple sclerosis (MS)?
ALS and MS are both neurological diseases, but they are very different. MS is an autoimmune disease where the immune system attacks the myelin sheath of nerves—it is usually relapsing-remitting and rarely fatal within the first decade. ALS destroys motor neurons directly; it does not involve the immune system attacking myelin. ALS is relentlessly progressive, while MS has a more variable course. Sensory symptoms are common in MS; they are rare in ALS.
What does Amyotrophic Lateral Sclerosis feel like in the early stages?
Early ALS is often subtle. Many patients first notice that one hand or foot is “just not working right” — they drop objects, trip on uneven ground, or notice a finger is harder to move. Fasciculations (muscle twitches visible under the skin) are common. Importantly, ALS is usually not painful in early stages—which is one reason it takes so long to diagnose.
Is Amyotrophic Lateral Sclerosis a painful death?
Most ALS patients do not experience severe pain. The primary cause of death — respiratory failure — can be peaceful with appropriate end-of-life care, including hospice support, opioids for air hunger, and benzodiazepines for anxiety. Good palliative care and early discussion of ventilator preferences dramatically improve the end-of-life experience. Medical cannabis also plays a growing role in comfort care during late-stage and end-stage ALS.
How fast does Amyotrophic Lateral Sclerosis progress after the first symptoms?
ALS progression varies widely. On average, patients progress from first symptoms to needing a wheelchair in 12–24 months and to respiratory involvement in 2–4 years. However, roughly 10% of patients — called “long-term survivors” — live 10 years or more (Stephen Hawking lived 55 years with ALS). Bulbar-onset ALS typically progresses faster than limb-onset ALS.
Can Amyotrophic Lateral Sclerosis be detected by an MRI?
MRI cannot diagnose ALS directly, but it is an essential diagnostic tool. Brain and spinal MRI rules out other causes of motor weakness (like a tumor or structural lesion). In some patients, MRI shows T2/FLAIR signal hyperintensity along the corticospinal tract — a finding suggestive of upper motor neuron degeneration. EMG remains the gold standard for confirming lower motor neuron involvement.
What is bulbar-onset Amyotrophic Lateral Sclerosis?
Bulbar-onset ALS begins with weakness in the muscles of speech and swallowing, controlled by the “bulbar” motor neurons in the brainstem. About 25–30% of ALS patients have bulbar onset. Symptoms include slurred speech (dysarthria), difficulty swallowing (dysphagia), excess saliva, and changes in voice quality. Bulbar-onset ALS tends to progress more rapidly and often requires augmentative communication devices and feeding tube placement earlier than limb-onset disease.
Is ALS a qualifying condition for medical cannabis in Florida?
Yes. ALS (amyotrophic lateral sclerosis) is a qualifying condition under Florida’s medical marijuana program. Patients with ALS can receive a medical marijuana certification from a licensed physician, enabling them to purchase cannabis from state-licensed dispensaries. Venice Care’s Dr. Barry Gordon provides these evaluations in Venice, FL and via telehealth. Contact us at venicecare.com to book an appointment.
Where can ALS patients find clinical trials in the USA?
The best resource is ClinicalTrials.gov — search “amyotrophic lateral sclerosis” and filter by “recruiting” and your state. The ALS Association’s online tool (als.org/research/clinical-trials) also helps match patients to open studies. Ask your neurologist or ALS multidisciplinary clinic about trials in your area.
Medical Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice and should not substitute for consultation with a licensed physician. Amyotrophic lateral sclerosis is a complex disease; diagnosis and treatment decisions must be made by qualified medical professionals. Venice Care provides medical cannabis evaluations within the scope of Florida law. For ALS emergencies, contact your neurologist or call 911.